

89 million masks, 30 million gowns, 2.9 million litres of hand sanitiser. A month.
- Written by: Katherine Gibney, NHMRC early career fellow, The Peter Doherty Institute for Infection and Immunity
In three short months, more than half a million cases of the novel coronavirus, COVID-19, have been reported worldwide.
The US now has the highest number of COVID-19 cases worldwide and Italy has reported more than twice as many COVID-19 related deaths as China. Deaths from COVID-19 in Spain have surpassed China in recent days, and it won’t be long before France and the US follow suit. COVID-19 has well and truly taken hold in the West.
While most people are being encouraged (or ordered) to stay at home to reduce the spread of COVID-19, this is not an option for frontline healthcare workers.
Healthcare workers have been infected at an alarming rate
In countries whose health infrastructure has been overwhelmed by the sheer volume of severe COVID-19 cases, healthcare workers have been infected at an alarming rate.
In Italy, more than 6,000 healthcare workers have been infected, making up 9% of the total COVID infections. In Spain, 17% of female COVID-19 cases are healthcare workers (12% of all COVID-19 cases are healthcare workers). More than 2,000 healthcare workers in China had laboratory confirmed COVID-19, with 88% occurring in the worst affected Hubei province.
In Australia, COVID-19 patients are cared for in single rooms where available. However, soon it will be necessary to care for COVID-19 patients in wards and ICUs alongside other COVID-19 patients – known as “cohorting” – as a patient with COVID-19 cannot catch the same disease from another patient sharing their ward.
COVID-19 is transmitted primarily by virus-containing droplets that are expelled when an infectious person sneezes, coughs or talks, contaminating others in close face-to-face proximity and nearby surfaces. This underlies the general advice to stay more than 1.5 metres away from others, practice good cough etiquette and hand hygiene, and avoid touching your face with your hands.
 Don’t hoard or panic-buy masks and other personal protective equipment.
AAP/EPA/JUSTIN LANE
Don’t hoard or panic-buy masks and other personal protective equipment.
AAP/EPA/JUSTIN LANE
The number of masks, goggles, gloves and gowns we’ll need is staggering
Healthcare workers use personal protective equipment (PPE) – masks, goggles, gloves and gowns – and clean surfaces to prevent transmission in hospital.
Some procedures that are required when caring for critically ill patients can generate smaller virus-containing particles called aerosols, which can be inhaled.
In circumstances where aerosols could be generated, PPE requirements include use of a respirator mask (also known as a P2 or N95 mask) and a negative room pressure, where a slight vacuum is created to prevent contaminated air escaping the room.
The volume of PPE required to deal with the COVID-19 pandemic is staggering.
The WHO has estimated frontline healthcare workers will require at least 89 million masks, 30 million gowns, 1.6 million goggles, 76 million gloves, and 2.9 million litres of hand sanitiser every month during the global COVID-19 response.
Hoarding and misuse of masks puts healthcare workers at risk
The WHO has also noted panic buying, hoarding and misuse of PPE are putting lives at risk from COVID-19 and other infectious diseases.
Healthcare workers are most at risk if they don’t use appropriate PPE when caring for a COVID-19 patient, such as before the COVID-19 infection has been recognised. This is how a number of unlucky Australian healthcare workers have already been infected with COVID-19 at work, including four from the Werribee Mercy Hospital in Melbourne’s outer west.
Early recognition of potential COVID-19 cases, and instituting precautions including isolation and use of PPE, will protect healthcare workers. Routine use of surgical masks in high-risk clinical settings such as emergency departments, ICUs and COVID-19 screening clinics is now recommended in many places.
PPE supplies in many countries have reportedly been exhausted, forcing healthcare workers to care for COVID-19 patients without adequate protection. Inappropriate and irrational use of PPE, including use of masks in situations where there is no risk of droplet or airborne transmission, accelerate consumption of a finite PPE supply.
The urgent work of securing more PPE
The federal, state and territory governments are working hard to secure enough PPE to prevent this scenario in Australia, including boosting domestic production and manufacturing capacity. Local industry has stepped up with companies previously making other products now making hand hygiene products and masks.
This is urgent work because it’s likely a rapid surge in COVID-19 cases would consume current PPE supplies quickly.
Crisis strategies being employed internationally to deal with mask shortages include prolonged use, re-use by a single healthcare worker, and use beyond the manufacturer designated shelf life, although these are not standard practice. Work is also taking place around sterilisation of masks for re-use by health care workers, which again is not standard practice.
Healthcare workers are also at risk if PPE is used incorrectly, due to inadequate training, inattention, or fatigue. Training healthcare workers in correct use of PPE is a critical part of our emergency response.
Like everyone else, healthcare workers are at risk outside work. In China, outside Hubei, the majority of healthcare workers’ infections could be traced to a confirmed COVID-19 case in the household. As community transmission of COVID-19 becomes more widespread in Australia, more healthcare workers will be infected at home and in the community.
 In several countries, military personnel are helping source and distribute PPE.
AAP/DPA/Jonas Güttler
In several countries, military personnel are helping source and distribute PPE.
AAP/DPA/Jonas Güttler
When healthcare workers can’t work
It’s vital the healthcare workforce is maintained for the duration of the pandemic. Perversely, some of the actions taken to prevent COVID-19 transmission might result in healthcare workers’ workplace absenteeism. Often healthcare workers would work through a mild upper respiratory tract infection, but with the current heightened awareness they might not be doing this. All healthcare workers are being encouraged to present for testing if they have fever or acute respiratory symptoms such as sore throat, cough and difficulty breathing. They are usually unable to return to work until a negative COVID-19 test result is received and symptoms have resolved. This can take several days.
If a healthcare worker is exposed to a COVID-19 case when not wearing PPE (meaning they spend more than 15 minutes face-to-face or more than two hours in the same room as a case), they will be classed as a close contact and will be home-quarantined and unable to work for 14 days after they were exposed.
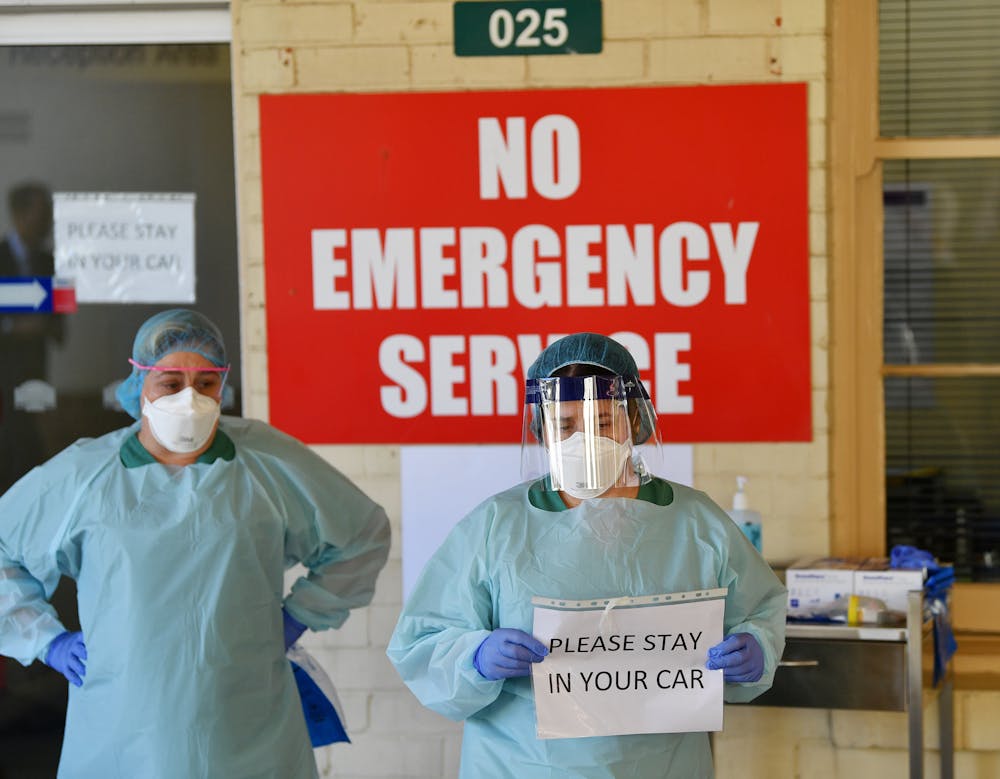 We must do everything we can to protect and support healthcare workers throughout this pandemic.
AAP/DAVID MARIUZ
We must do everything we can to protect and support healthcare workers throughout this pandemic.
AAP/DAVID MARIUZ
And carer responsibilities – either for someone unwell with COVID-19 or for children unable to attend childcare or school due to closures – will keep many healthcare workers away from work.
In the current climate, healthcare workers have been described as “every country’s most valuable resource.” Governments, employers and the public need to do everything they can to protect and support healthcare workers throughout this pandemic.
Read more: Why coronavirus may forever change the way we care within families
Authors: Katherine Gibney, NHMRC early career fellow, The Peter Doherty Institute for Infection and Immunity


















