

Want to quit a bad habit? Here's one way to compare treatments
- Written by: Sabine Braat, Biostatistician, University of Melbourne
This article is in the series This is research, where we ask academics to share and discuss open access articles that reveal important aspects of science.
Today’s piece explains the term “number needed to treat” or NNT. It’s a way to get a sense of whether the treatment you’re considering is likely to have an impact or not.
Whether it’s quitting smoking, reducing alcohol intake or making healthier dietary choices, many of us have habits we’d like to change. But it’s really hard to know which treatment path to take.
To advise their patients on the best of course of action, doctors sometimes compare treatments using something called the “number needed to treat” (NNT).
In deciding whether to embark on a course of treatment, NNT can help. But the term is easily misunderstood by patients, and doctors as well.
So it’s useful to break down what NNT means.
Read more: Trust Me, I'm An Expert: What research says about how to stick to your New Year’s resolutions
Comparing treatments
The NNT is a measure used to compare the benefits and harms of treatments. It was developed by three epidemiologists about 30 years ago.
Doctors like it for a couple of reasons:
- it’s easy to calculate
- it allows doctors to describe the effect of a treatment in terms of the number of patients that need to be treated in order to help one additional patient.
To understand how, let’s imagine we are running a randomised controlled trial to compare the effect of two different treatments intended to help smokers quit. Quitting smoking is notoriously hard, even with good intentions.
Read more: Randomised control trials: what makes them the gold standard in medical research?
Study participants are randomly assigned to a prescribed treatment (for example, a drug, let’s call it “NoSmoke”) or some minimal behavioural support (such as counselling).
Suppose we find that 16.5% of the smokers who received NoSmoke stopped smoking, while only 7.5% of those who received counselling quit.
It would seem obvious to compare these treatments by looking at the difference between these two percentages. Since 16.5% is greater than 7.5% (by 9%!), we could conclude that NoSmoke is more beneficial than counselling in helping people to stop smoking.
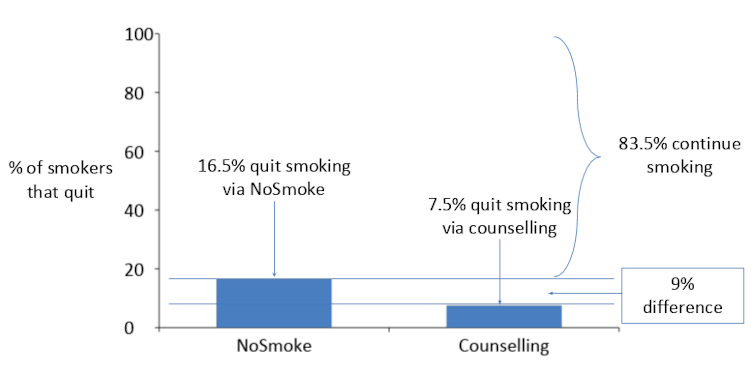 Looking at the percentages of smokers that quit, NoSmoke seems to be more effective than counselling.
Karen Lamb and Sabine Braat, Author provided
Looking at the percentages of smokers that quit, NoSmoke seems to be more effective than counselling.
Karen Lamb and Sabine Braat, Author provided
Although the difference in percentages is a useful way to compare the effect of treatments it can be tricky to interpret because it is abstract: it involves a probability. In our example, the probability for a person to stop smoking increases from 7.5% with counselling to 16.5% with NoSmoke.
The NNT gives us an alternative way to understand the impact of a treatment.
Real outcomes for patients
In this smoking example, the NNT helps you see how many patients need to receive a stop smoking treatment (compared to another treatment) for one more patient to stop smoking.
Read more: Why Australian prisoners are smoking nicotine-infused tea leaves
The NNT is obtained by dividing 100% by the difference in percentages of patients with the outcome. In our example above, the NNT is about 11 (100 divided by 9 – since 16.5 minus 7.5 is 9). This means that to have one additional smoker quitting, on average 11 smokers need to use NoSmoke (rather than receive minimal behavioural support).
A higher NNT means that more patients need to receive the new treatment in order for one additional patient to reach the outcome compared to the reference treatment.
Nicotine replacement therapy
Let’s look at some real data. In a large review paper published in 2016, the NNT for all types of nicotine replacement therapy was reported to be 23. This means that on average 23 smokers need to receive nicotine replacement therapy – such as a patch, gum, or lozenge – for one additional smoker to quit (compared to behavioural support only).
Comparing this value with our hypothetical clinical trial NoSmoke data presented above, we can quickly see that the use of NoSmoke (which had an NNT of 11) is about 2 times more likely to result in quitting than use of nicotine replacement therapy.
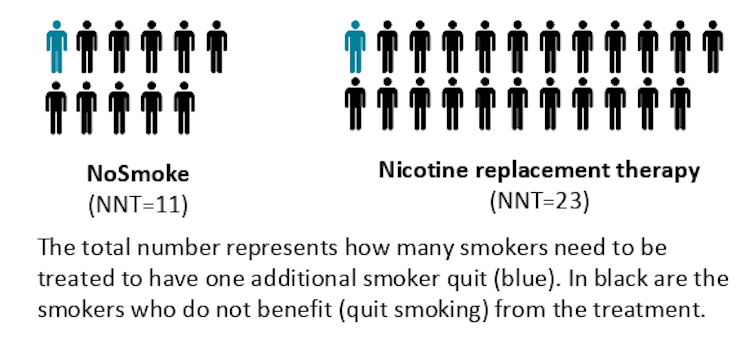 NNT values show how many people need to be treated in order for a treatment to be effective for one person.
Karen Lamb and Sabine Braat, Author provided
NNT values show how many people need to be treated in order for a treatment to be effective for one person.
Karen Lamb and Sabine Braat, Author provided
The ideal NNT for treatment benefit is 1, in which case every single patient on the new treatment should benefit from receiving this new treatment.
The NNT can express both benefits and harms. For instance, the NNT for heart palpitations or chest pains with nicotine replacement therapy is 94: this means on average 94 persons would have to use nicotine replacement therapy to observe one additional person with a harmful outcome (heart palpitations or chest pains).
Understanding the NNT
While the use of NNT is widespread, it has been reported that the NNT is actually frequently misunderstood by patients and doctors alike.
In addition, shortcomings of the NNT are well described in the scientific literature. The NNT varies with the risk of the outcome under the reference treatment (in our example this is the “risk” of stopping smoking for those that received counselling) and depends on duration of treatment and follow-up. These factors should be similar between studies when comparing NNTs.
The NNT may claim to be a helpful way to compare treatments quickly, however measures such as the difference in percentages may actually be easier to grasp and less likely to mislead both patient and doctor.
The open access research paper referred to in this analysis is Nicotine receptor partial agonists for smoking cessation.
Authors: Sabine Braat, Biostatistician, University of Melbourne
Read more http://theconversation.com/want-to-quit-a-bad-habit-heres-one-way-to-compare-treatments-109144


















